Mie Sonomoto
About the department
In Pediatric Dentistry, we provide prevention and treatment of dental caries and periodontal disease, treatment for teeth alignment, surgical procedures for impacted extra teeth and cysts, treatment of dental/oral injuries, and the guidance on eating function for impaired development of oral functions. Unexpected abnormalities or diseases may occur from the lactation period to the time when all permanent teeth come in. In order to detect and treat them at an early stage, we perform periodic oral management from the age of 0 to 18 years at our department aiming at extension of healthy life expectancy in the future.
- Facility certified by academic societies
- Certified training facility of the Japanese Society of Pediatric Dentistry
- Certified facility for clinical experience of the Japanese Society for Disability and Oral Health
Common oral diseases treated
- Dental caries (including early stage of dental caries)
- Gum disease
- Teeth alignment
- Dental trauma
- Disease required oral surgery (extra tooth, dentigerous cyst, oral mucocele, etc.)
- Tooth abnormalities (number, shape, color, timing of growth, etc.)
- Impaired development of oral functions
Director of the department

Specialty/qualification
- Board certified specialist and instructor of the Japanese Society of Pediatric Dentistry
- JSDH-certified dentist
(JSDH: Japanese Society for Disability and Oral Health) - Board certified dental clinical instructor of the Japan Association of Dental Traumatology
Chief Dental Clinician
Yoko Abe
Specialty/qualification
- Board certified specialist and instructor of the Japanese Society of Pediatric Dentistry
- JSDH-certified dentist and consultant
(JSDH: Japanese Society for Disability and Oral Health)
Characteristics of dental care
1. Management of initial dental caries
In the mouth, demineralization and remineralization are repeated: eating food or drinking beverages makes the inside of the mouth acidic (demineralization of teeth), and then saliva makes it neutral (remineralization of teeth) after eating. Dental caries is loss of tooth substance that begins with demineralization of the tooth surface layer (enamel). The visible hole in a tooth as a result of progression of dental caries is called a "caries cavity." It is necessary to drill and fill the tooth at this stage because natural healing does not occur. When dental caries progresses to dentine, symptoms such as pain appear. However, initial dental caries is asymptomatic and difficult to notice. Therefore, it is effective to have a periodical checkup at a dental clinic to have initial dental caries discovered at an early stage, to naturally heal initial dental caries by remineralization such as the application of fluoride, and to prevent the progression of dental caries. Children are most likely to develop dental caries in both primary teeth and permanent teeth during the first few years after they come in due to weak tooth quality. In our department, we conduct dental checkup every 3 months to prevent the development of new caries cavities, and the specialists clean the teeth, apply high concentration fluoride, and give lifestyle guidance mainly on dietary habits. We recommend that children have dental checkup from the time when there are no caries cavities.
2. Treatment of dental caries of anterior primary teeth
Dental caries with cavities should be treated even in primary teeth because they cause dental caries in permanent teeth or cause bad dentition. In particular, dental caries of anterior primary teeth are noticed by friends. Since children have less dental caries in primary teeth now, we think that dental caries should be treated to restore the original state as much as possible from the perspective of psychological development and thus provide restoration procedures.



3. Short time treatment without drilling tooth for children with high anxiety (Atraumatic Restorative Treatment: ART)
In recent years, it has been recognized that sealing caries cavities with glass ionomer cement (GIC) greatly reduces bacteria and softened tooth substance is remineralized. In our department, we just scrape a little dirt from the caries cavities with a hand tool without drilling teeth and close numerous caries cavities with GIC for children who cry for the fear of dental treatment. After that, we conduct periodical dental checkups, mainly guidance of brushing and diet and application of fluoride until children become accustomed to a dental checkup. When they finally become less anxious, we will provide final treatment for dental caries. We attentively conduct dental examination so that children do not hate dentists.

Many severe dentine dental caries
Hand tools

Finishing by filling GIC in many caries cavities in a few minutes
4. Treating dental trauma
Dental trauma are common in childhood. They occur most frequently between the ages of 1 to 3 years with primary teeth and 7 to 9 years with permanent teeth. Symptoms include breaking of teeth (fracture), changes in the position or length of teeth (dislocation), and loss of teeth (avulsion), and each is treated with different procedure. It is recommended to see a dentist as soon as possible after dental trauma. If you have a tooth broken, bring “a chip of tooth” with you. In the case of avulsion, “soak a tooth in milk” and bring it with you.
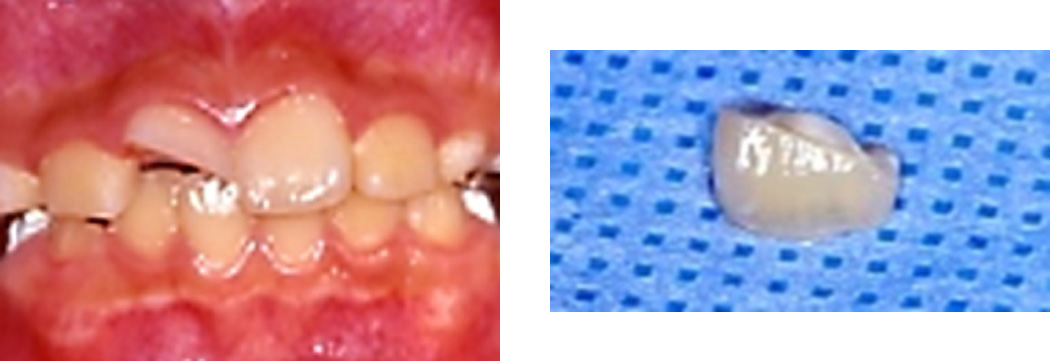
Fracture of a permanent tooth crown and a chip of the tooth

Dislocation of primary teeth

Avulsion of a permanent tooth
5. Pediatric surgical treatment
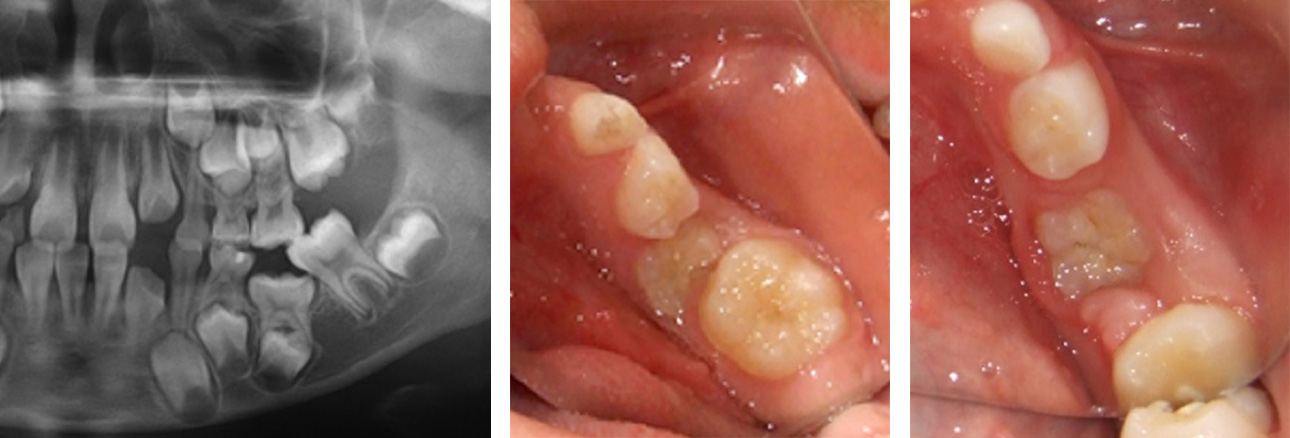
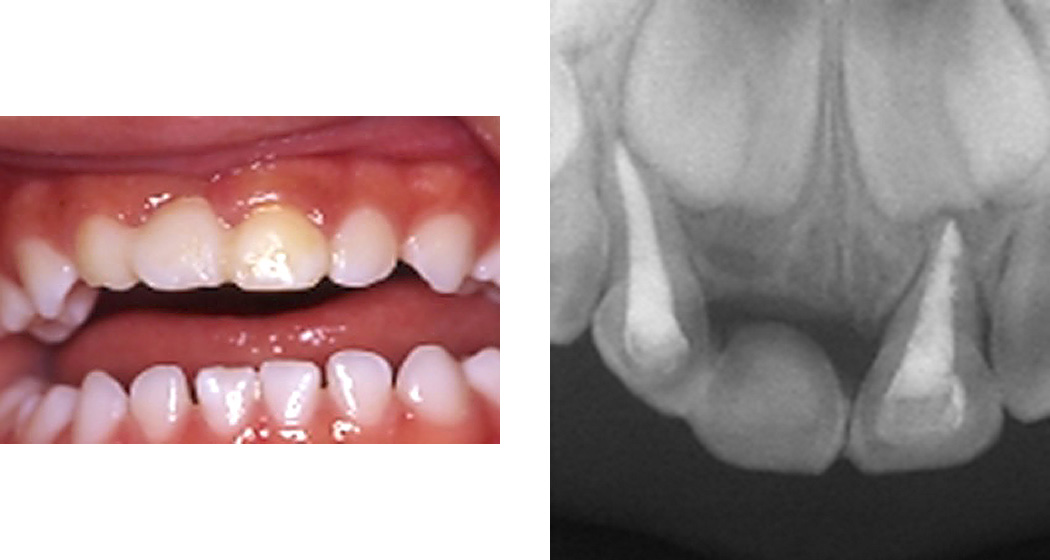
1) Extraction of extra teeth


It is difficult to detect the abnormality on the intraoral photograph, but two extra teeth (white and black arrows) are observed on the X-ray photo. These extra teeth should be extracted at an appropriate timing because they may interfere with the growth of a permanent tooth. In our department, we usually perform extraction under local anesthesia but perform under general anesthesia in some cases.
2) Removal of oral mucocele

A swelling or bump sometimes appears on the mucosa of the lower lip. It is called oral mucocele, accumulation of saliva, caused by a blocked salivary gland. It is removed by surgery under local anesthesia.
6. Teeth alignment
It is important to detect factors that interfere with occlusal development early and perform occlusal management from the primary dentition period so that healthy dentition and occlusion are expected to be achieved in permanent dentition.
1) Cross bite
In our department, we believe that underbite of primary teeth should be treated if possible, and we start treatment with a simple device in children aged around 3 to 5 years.

Underbite (before treatment)
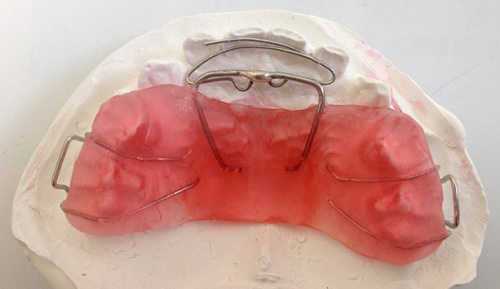
Removable device

After treatment
2) Premature loss of primary teeth
If primary teeth are lost at an early stage due to dental caries, etc. and they are left untreated, the existing permanent teeth may incline or a site for an unerupted permanent tooth may be lost. To prevent them, we apply a space retention device that keeps a gap to guide normal replacement. (lingual arch, band-loop space maintainer, etc.)

Lingual arch

Band-loop
3) Abnormal eruption site of primary teeth (submerged primary teeth)
Primary teeth may stop growing halfway (called submerged primary teeth). If a submerged primary tooth is left untreated, abnormalities occur to the alignment of the permanent teeth. Thus, it has to be extracted. Before extraction, it is often necessary to move a back tooth first to create space for extraction.
Submerged primary tooth

Extracted submerged primary tooth
7. Support for development of eating and swallowing function in children with Down syndrome
In many children with Down syndrome, oral functions delay in development due to muscle hypotonia, which results in eating and swallowing disorders, such as not eating baby food, swallowing food without chewing, or eating while protruding the tongue. Some Down syndrome children are fed with a nose or gastrostomy tube due to poor suckling. In our department, we give development guidance for eating and swallowing functions. It is known that better results can be obtained by intervention from children as young as possible. Therefore, it is recommended to visit us at the time of starting weaning.
Efforts for state-of-the-art dental care
1. New dental caries testing method
1) Oral cleanliness indicator (Cariscreen)
We have introduced a testing method that can quantify the cleaning status of the oral cavity. It takes only about 75 seconds to get a result.
Cariscreen
2) Optical dental caries testing device (DIAGNOdent pen)
We have introduced a small instrument capable of visualizing initial dental caries, which is macroscopically difficult to assess, with a laser light. Changes in the mouth can be recorded with objective values by periodical measurement.

DIAGNOdent pen
Oral photograph and X-ray image after treatment